Atrioventricular nodal reentrant tachycardia (AVNRT) and atrioventricular reentrant tachycardia (AVRT) are two types of supraventricular tachycardias (SVTs) that affect the heart's rhythm. While both conditions involve abnormal electrical pathways in the heart, they have distinct differences in terms of their underlying mechanisms, symptoms, and treatment approaches. In this article, we will delve into the differences between AVNRT and AVRT, exploring their causes, characteristics, and management strategies.
Key Points
- AVNRT and AVRT are two distinct types of supraventricular tachycardias (SVTs) with different underlying mechanisms.
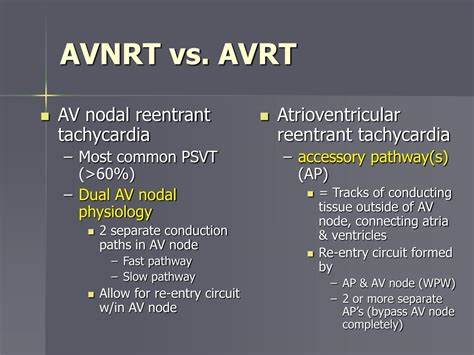
- AVNRT is characterized by a reentrant circuit within the atrioventricular (AV) node, whereas AVRT involves an accessory electrical pathway between the atria and ventricles.
- Symptoms of AVNRT and AVRT can be similar, but AVRT is more commonly associated with underlying heart disease.
- Treatment approaches for AVNRT and AVRT differ, with AVNRT often managed with vagal maneuvers or adenosine, and AVRT typically requiring catheter ablation or medication.
- Accurate diagnosis and differentiation between AVNRT and AVRT are crucial for effective management and prevention of complications.
Underlying Mechanisms and Characteristics

AVNRT is a type of SVT that occurs when there is a reentrant circuit within the atrioventricular (AV) node. The AV node is a critical structure in the heart that regulates the electrical signals between the atria and ventricles. In AVNRT, the reentrant circuit creates a self-sustaining loop of electrical activity that can cause the heart to beat rapidly. AVNRT is often triggered by stress, anxiety, or other factors that stimulate the heart.
On the other hand, AVRT is a type of SVT that involves an accessory electrical pathway between the atria and ventricles. This accessory pathway, also known as a bypass tract, can allow electrical signals to bypass the AV node and directly stimulate the ventricles. AVRT can be further divided into two subtypes: orthodromic AVRT, where the electrical signal travels down the accessory pathway and then back up to the atria through the AV node, and antidromic AVRT, where the signal travels down the accessory pathway and then back up to the atria through another accessory pathway.
Symptoms and Clinical Presentation
The symptoms of AVNRT and AVRT can be similar, including palpitations, shortness of breath, chest pain, and dizziness. However, AVRT is more commonly associated with underlying heart disease, such as Wolff-Parkinson-White syndrome, which is a condition characterized by the presence of an accessory electrical pathway. AVRT can also be more likely to cause significant hemodynamic instability, particularly in patients with underlying heart disease.
In contrast, AVNRT is often seen in patients without underlying heart disease and may be triggered by stress, anxiety, or other factors that stimulate the heart. AVNRT can also be more responsive to vagal maneuvers, such as the Valsalva maneuver or carotid massage, which can help to terminate the arrhythmia.
| Characteristics | AVNRT | AVRT |
|---|---|---|
| Underlying Mechanism | Reentrant circuit within the AV node | Accessory electrical pathway between atria and ventricles |
| Symptoms | Palpitations, shortness of breath, chest pain, dizziness | Palpitations, shortness of breath, chest pain, dizziness, hemodynamic instability |
| Association with Heart Disease | Less common | More common, particularly with Wolff-Parkinson-White syndrome |
| Response to Vagal Maneuvers | Often responsive | Less responsive |

Treatment Approaches

The treatment approaches for AVNRT and AVRT differ. AVNRT is often managed with vagal maneuvers, such as the Valsalva maneuver or carotid massage, which can help to terminate the arrhythmia. Adenosine, a medication that can help to slow the heart rate, is also commonly used to treat AVNRT. In some cases, catheter ablation may be necessary to destroy the reentrant circuit within the AV node.
In contrast, AVRT is typically managed with catheter ablation or medication. Catheter ablation involves the use of a catheter to destroy the accessory electrical pathway, which can help to prevent the arrhythmia from recurring. Medications, such as beta blockers or anti-arrhythmic agents, may also be used to help control the heart rate and prevent recurrence of the arrhythmia.
Conclusion and Future Directions
In conclusion, AVNRT and AVRT are two distinct types of supraventricular tachycardias with different underlying mechanisms, symptoms, and treatment approaches. While both conditions can cause significant symptoms and hemodynamic instability, accurate diagnosis and differentiation between the two conditions are crucial for effective management and prevention of complications. Further research is needed to improve our understanding of the underlying mechanisms and to develop more effective treatment strategies for these conditions.
What is the main difference between AVNRT and AVRT?
+The main difference between AVNRT and AVRT is the underlying mechanism. AVNRT involves a reentrant circuit within the AV node, whereas AVRT involves an accessory electrical pathway between the atria and ventricles.
How are AVNRT and AVRT diagnosed?
+AVNRT and AVRT are diagnosed using a combination of electrocardiogram (ECG), echocardiogram, and other diagnostic tests. A thorough medical history and physical examination are also essential for accurate diagnosis.
What are the treatment options for AVNRT and AVRT?
+The treatment options for AVNRT and AVRT differ. AVNRT is often managed with vagal maneuvers or adenosine, while AVRT is typically managed with catheter ablation or medication.
Meta Description: Learn about the differences between AVNRT and AVRT, two types of supraventricular tachycardias, and understand their underlying mechanisms, symptoms, and treatment approaches.